Prescribe Acthar Gel now
Start the referral process for your appropriate patients
Nelson WW, Lima AF, Kranyak J, Opong-Owusu B, Ciepielewska G, Gallagher JR, Heap K, Carroll S—Journal of Ocular Pharmacology and Therapeutics, 2019
Disclosure statement: Funding to support this study was provided by Mallinckrodt Pharmaceuticals.
To describe patient characteristics, utilization patterns of Acthar Gel and concomitant therapies, and physicians' assessments of Acthar Gel treatment effects on patients' health status
Patient population
Baseline patient and disease characteristics (N=91)
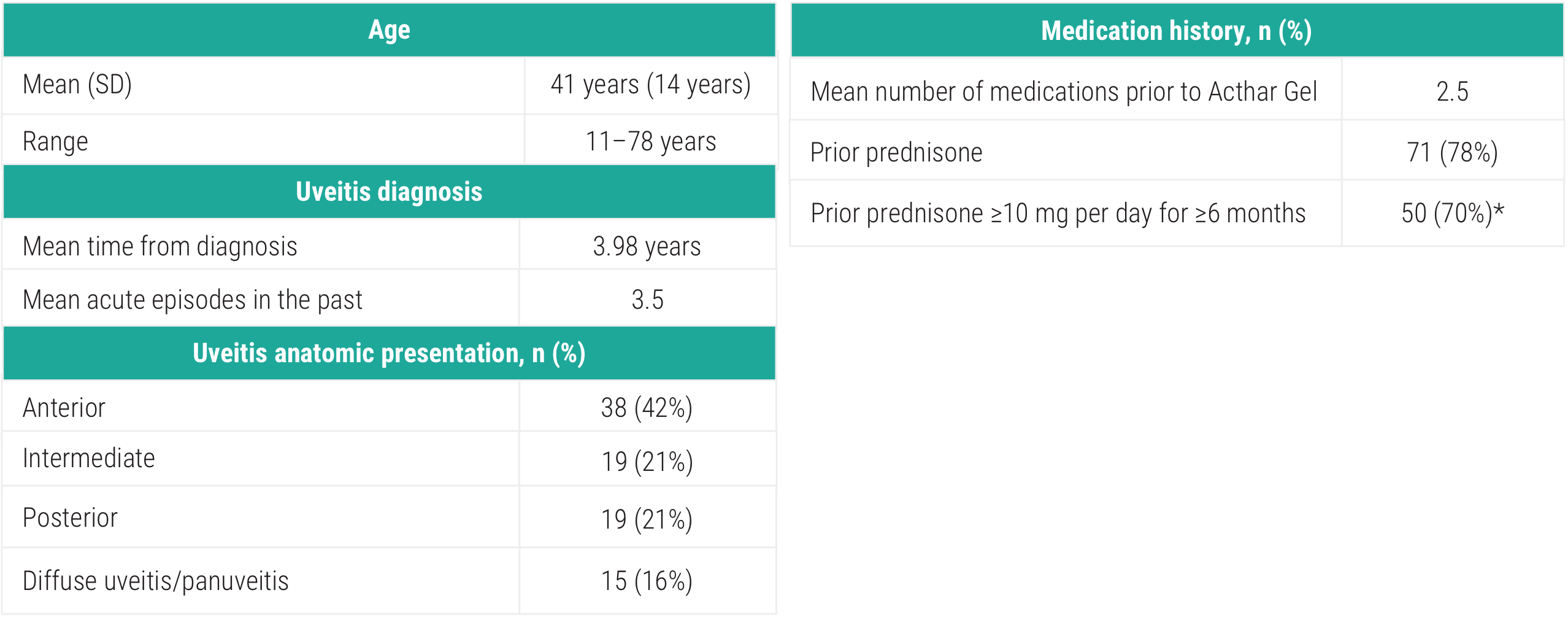
SD=standard deviation.
*Among 71 patients with documented prednisone treatment.
Baseline visual impairment level, n (%)
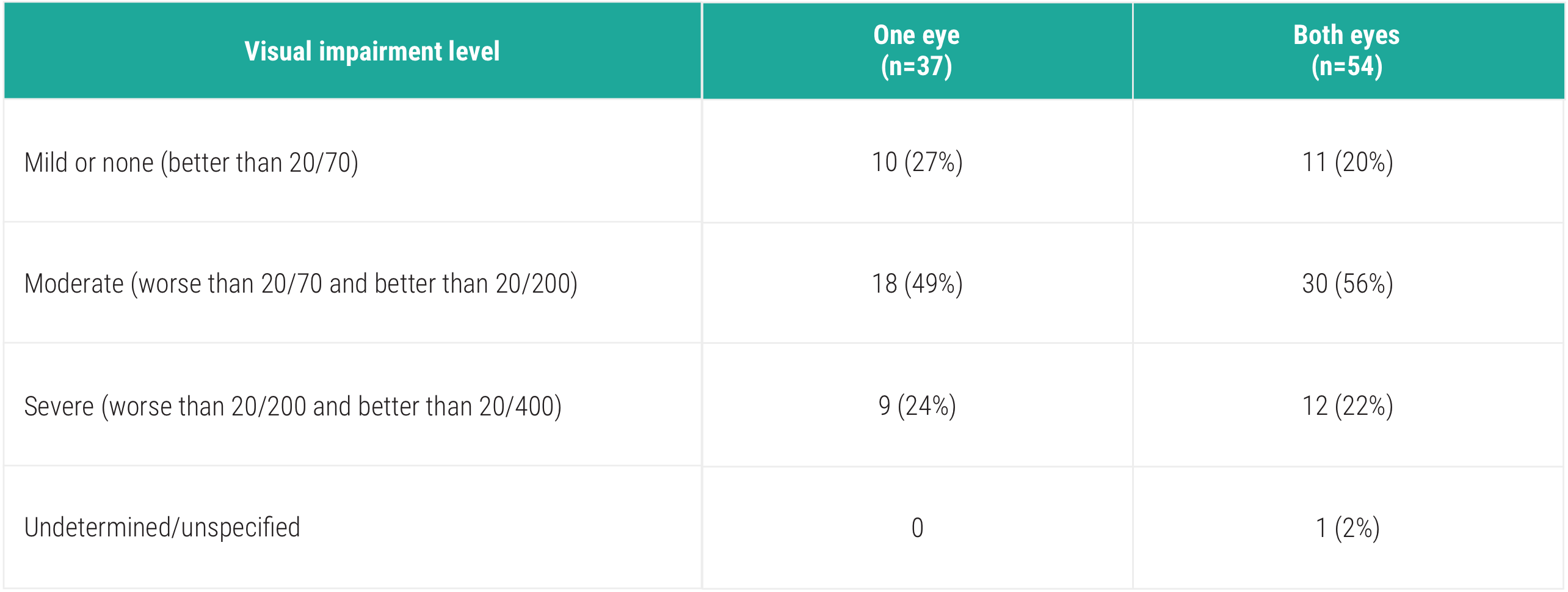
No patients were considered blind according to World Health Organization and ICD-10 criteria.
Uveitis symptoms and severity before initiation of Acthar Gel (N=91)
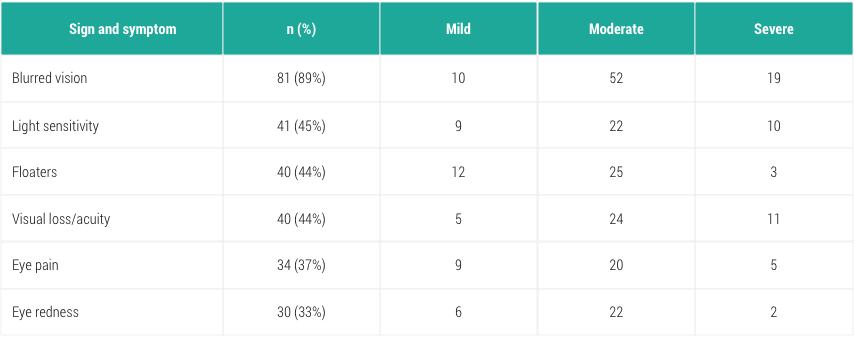
Available options included all those shown in the table. Respondents could select all options that applied; sum exceeds 100%.
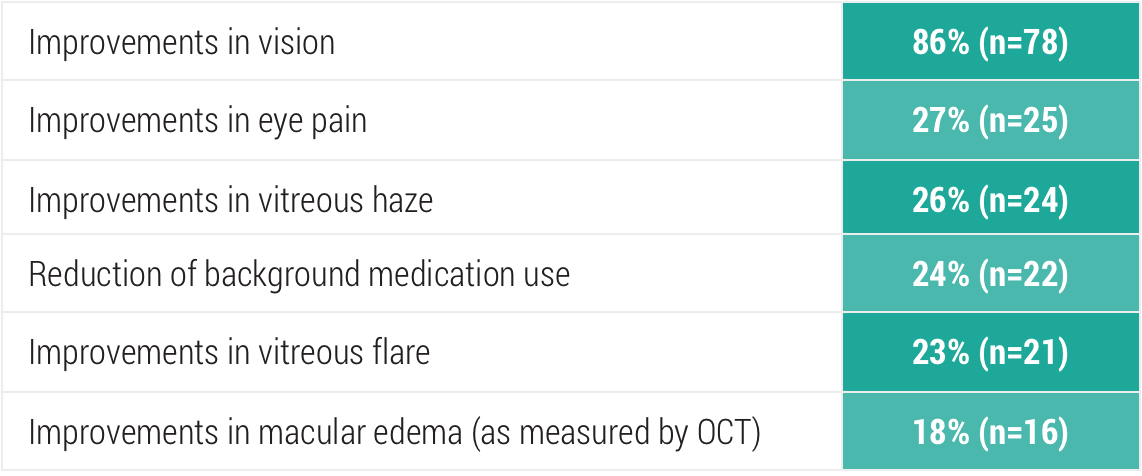
Clinical outcomes may not be solely attributable to Acthar Gel.
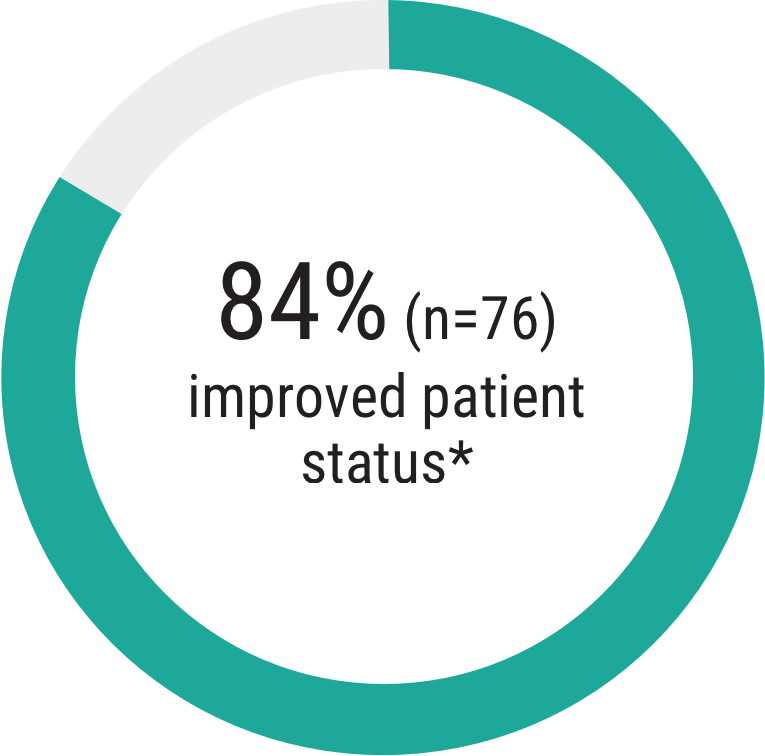
Patient status remained the same: 16% (n=15)
OCT=optimal coherence tomography.
*Based on physicians' responses to the following two prompts:
Patient status remained the same: 16% (n=15)
Co-medication use in patients with uveitis 3 months
before, during,
and 3 months after treatment
with Acthar Gel1
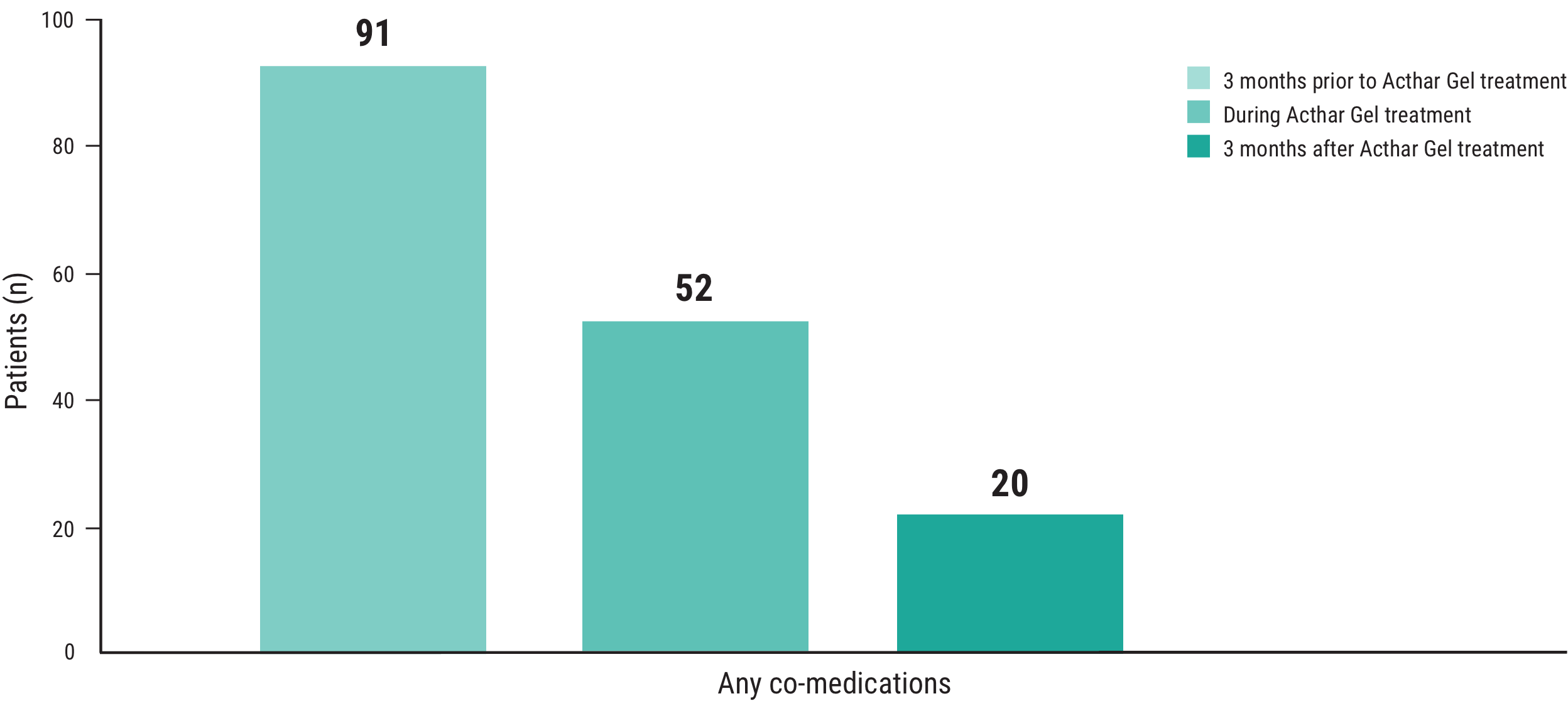
Clinical outcomes may not be solely attributable to Acthar Gel.
Start the referral process for your appropriate patients

See additional dosing information from clinical experience with Acthar Gel
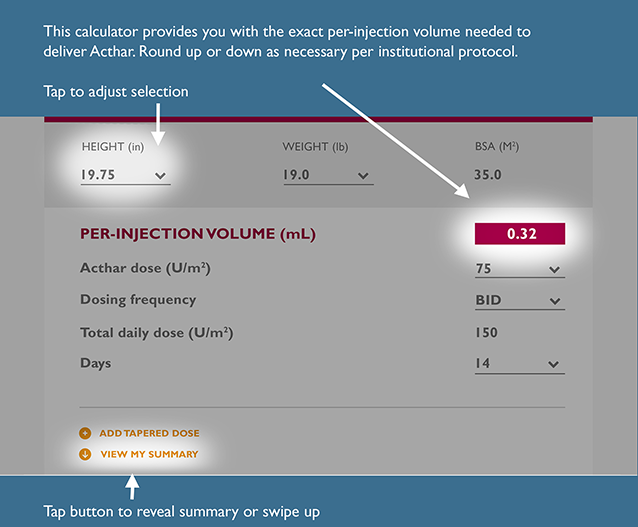
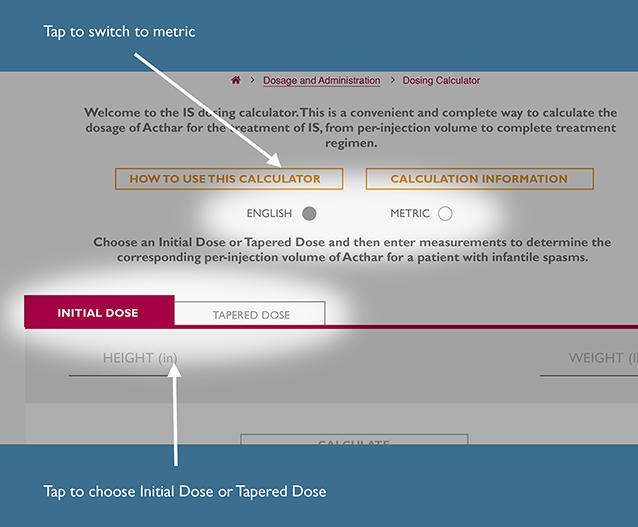
This is a convenient and complete way to calculate the recommended dosage of Acthar Gel for the treatment of IS, from per-injection volume to a complete treatment regimen.
The recommended dosage for IS is 150 units/m2 divided into twice daily intramuscular injections of 75 units/m2 over a 2‑week period. Dosing should be gradually tapered and discontinued over a 2‑week period.
Choose initial dose or tapered dose and then enter measurements to determine the corresponding per-injection volume of Acthar Gel for a patient with IS.
INITIAL DOSE
TAPERED DOSE #1
For Infantile Spasms, the Acthar IS Dosing Calculator generates per-injection volume (mL) of Acthar by body surface area (BSA) using the following Mosteller formula calculation22:
To determine per-injection volume of Acthar:
To determine total daily dose:
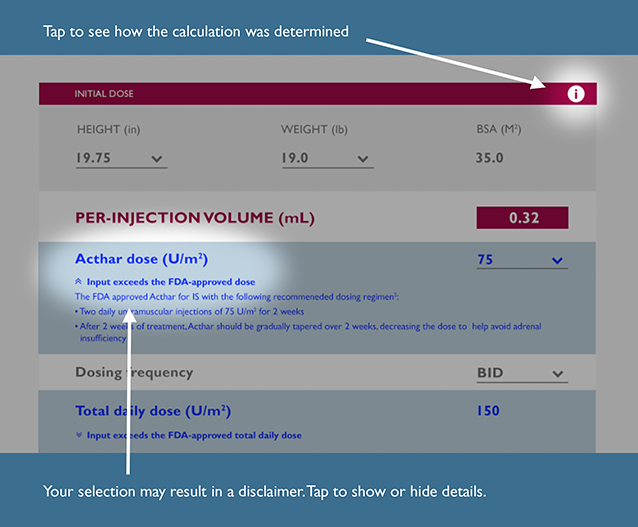
Input exceeds the FDA-recommended dose
The FDA approved Acthar for IS with the following recommended dosing regimen1:
Input is below the FDA-recommended dose
The FDA approved Acthar for IS with the following recommended dosing regimen1:
Input exceeds the preceding total daily dose
After 2 weeks of treatment, Acthar should be gradually tapered, decreasing the dose to help avoid adrenal insufficiency. The FDA approved Acthar for IS with the following recommended taper schedule1:
30 U/m2 in the morning for 3 days; 15 U/m2 in the morning for 3 days; 10 U/m2 in the morning for 3 days; and 10 U/m2 every other morning for 6 days.
The previous dose is outside the FDA-approved recommendation for dose range; therefore, the default taper dose may need assessment
After 2 weeks of treatment, Acthar should be gradually tapered, decreasing the dose to help avoid adrenal insufficiency. The FDA approved Acthar for IS with the following recommended taper schedule1:
30 U/m2 in the morning for 3 days; 15 U/m2 in the morning for 3 days; 10 U/m2 in the morning for 3 days; and 10 U/m2 every other morning for 6 days.
Input differs from the FDA-recommended frequency of treatment
The FDA approved Acthar for IS with the following recommended dosing regimen1:
Input differs from the FDA-approved tapering schedule recommendation
After 2 weeks of treatment, Acthar should be gradually tapered, decreasing the dose to help avoid adrenal insufficiency. The FDA approved Acthar for IS with the following recommended taper schedule1:
30 U/m2 in the morning for 3 days; 15 U/m2 in the morning for 3 days; 10 U/m2 in the morning for 3 days; and 10 U/m2 every other morning for 6 days.
The symptoms of adrenal insufficiency in infants treated for infantile spasms can be difficult to identify. The symptoms are non-specific and may include anorexia, fatigue, lethargy, weakness, excessive weight loss, hypotension and abdominal pain. It is critical that parents and caregivers be made aware of the possibility of adrenal insufficiency when discontinuing Acthar Gel and should be instructed to observe for, and be able to recognize, these symptoms.
Input exceeds the preceding total daily dose
After 2 weeks of treatment, Acthar should be gradually tapered, decreasing the dose to help avoid adrenal insufficiency. The FDA approved Acthar for IS with the following recommended taper schedule1:
30 U/m2 in the morning for 3 days; 15 U/m2 in the morning for 3 days; 10 U/m2 in the morning for 3 days; and 10 U/m2 every other morning for 6 days.
Input exceeds the preceding total daily dose
After 2 weeks of treatment, Acthar should be gradually tapered, decreasing the dose to help avoid adrenal insufficiency. The FDA approved Acthar for IS with the following recommended taper schedule1:
30 U/m2 in the morning for 3 days; 15 U/m2 in the morning for 3 days; 10 U/m2 in the morning for 3 days; and 10 U/m2 every other morning for 6 days.
Input exceeds the FDA-recommended total daily dose
The FDA approved Acthar for IS with the following recommended dosing regimen1:
Please note that there are no data to support the use of Acthar at a total daily dose exceeding 150 U/m2. This dosing calculator is not a substitute for clinical judgment. Medical discretion is required to determine any appropriate daily dose and treatment course of Acthar for your IS patients.
Input is below the FDA-recommended total daily dose
The FDA approved Acthar for IS with the following recommended dosing regimen1:
Input differs from the FDA-recommended days on therapy
The FDA approved Acthar for IS with the following recommended dosing regimen1:
Input differs from the FDA-approved tapering schedule recommendation
After 2 weeks of treatment, Acthar should be gradually tapered, decreasing the dose to help avoid adrenal insufficiency. The FDA approved Acthar for IS with the following recommended taper schedule1:
30 U/m2 in the morning for 3 days; 15 U/m2 in the morning for 3 days; 10 U/m2 in the morning for 3 days; and 10 U/m2 every other morning for 6 days.
The symptoms of adrenal insufficiency in infants treated for infantile spasms can be difficult to identify. The symptoms are non-specific and may include anorexia, fatigue, lethargy, weakness, excessive weight loss, hypotension and abdominal pain. It is critical that parents and caregivers be made aware of the possibility of adrenal insufficiency when discontinuing Acthar Gel and should be instructed to observe for, and be able to recognize, these symptoms.
ADD TAPERED DOSE
REMOVE THIS DOSE
VIEW MY SUMMARY
For infantile spasms, the Acthar IS Dosing Calculator generates per-injection volume (mL) of Acthar by body surface area (BSA) using the following Mosteller formula calculation22:

To determine per-injection volume of Acthar:

To determine total daily dose:
To determine total volume of Acthar required to complete your selected course of treatment:

To determine number of vials needed:

Download and fill out the Doctor Notification Letter to share your patient's prescription with their other healthcare providers.
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References: