Prescribe Acthar Gel now
Start the referral process for your appropriate patients
Kaplan J, Miller T, Baker M, Due B, Zhao E—Frontiers in Neurology, 2020
Disclosure statement: Funding to support this study was provided by Mallinckrodt Pharmaceuticals.
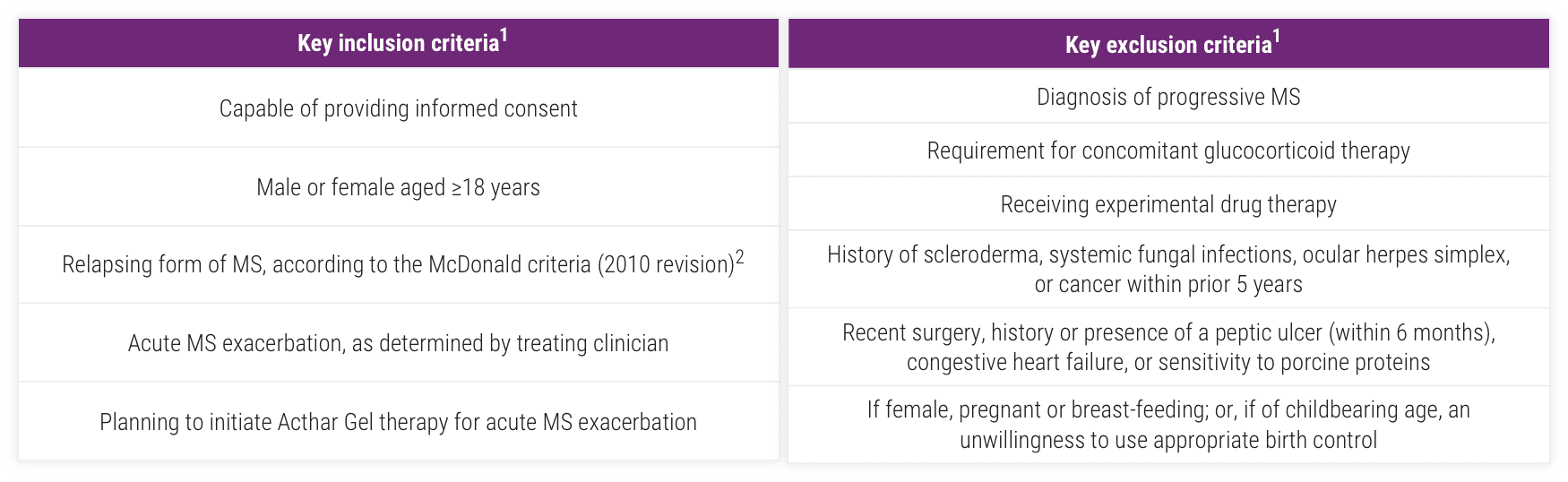
To characterize the patient population receiving Acthar Gel for the treatment of acute MS relapse and describe their treatment patterns, MS exacerbation recovery, and safety outcomes
AE=adverse event; EDSS=Expanded Disability Status Scale; ITT=intent-to-treat; MSIS-29v1=Multiple Sclerosis Impact Scale Version 1; SAE=serious adverse event.
*Demographics, medical history, disease-modifying therapies (DMTs) (prior 2 years), and concomitant medications collected at study enrollment as well as MSIS-29v1 and EDSS.
Baseline characteristics of patients who received Acthar Gel1
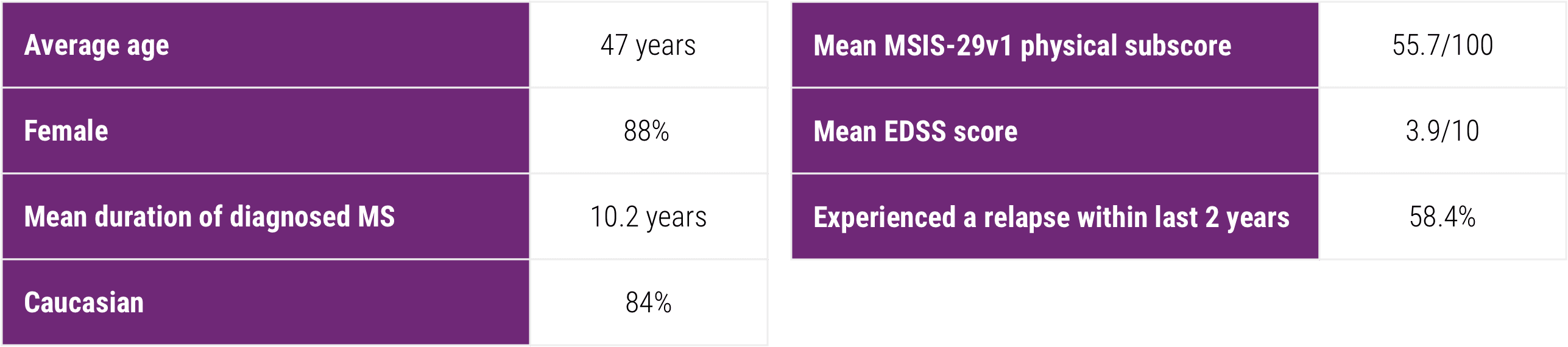
Approximately two-thirds of the patients reported using concomitant DMTs at some point during the study period
Percentage of patients that had a physician-reported history of a lack of sufficient treatment response, intolerance due to side effects, or IV access problems associated with previous treatment with high-dose glucocorticoids (eg, IVMP) for an MS relapse
IV=intravenous; IVMP=intravenous methylprednisolone.
Some patients with MS relapses experiencing recurring disease achieved clinically meaningful improvements in the MSIS-29v1 at 2 months—and sustained them at 6 months1,3,4
Mean change from baseline in the MSIS-29v1 scale1
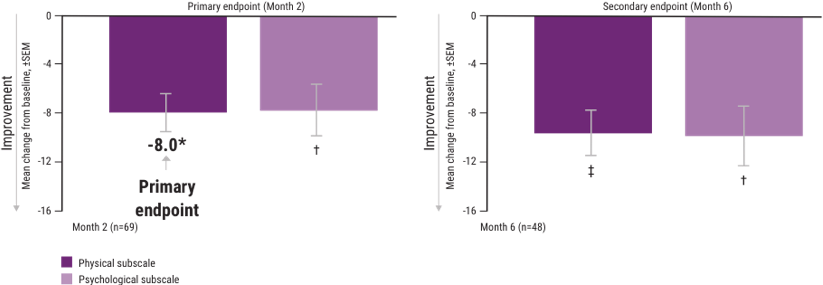
A change in score of ≥8 on the physical scale is considered clinically meaningful.5,6
ITT=intent-to-treat; MSIS-29v1=Multiple Sclerosis Impact Scale Version 1; SEM=standard error of the mean.
*P<.001.
†P<.01.
‡P<.0001.
Note: P values are based on Wilcoxon signed rank tests (ITT population) compared with baseline.
CGI-I=Clinical Global Impressions-Improvement; EDSS=Expanded Disability Status Scale.
Mean change from baseline in the EDSS scale1
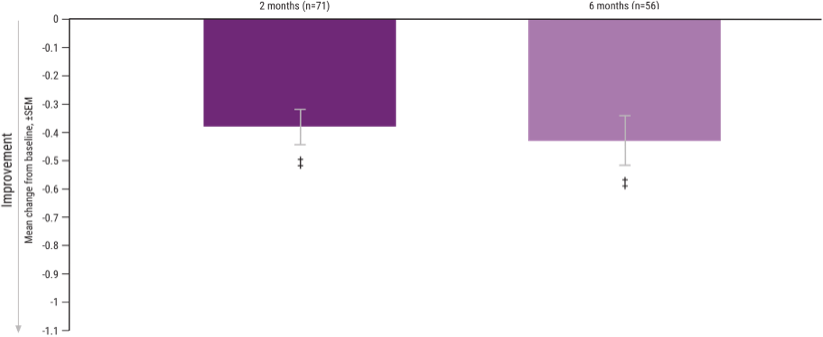
Mean scores decreased at 2 and 6 months from a baseline EDSS score of 3.9.
‡P <.0001.
Note: P values are based on Wilcoxon signed rank tests (ITT population) compared with baseline.
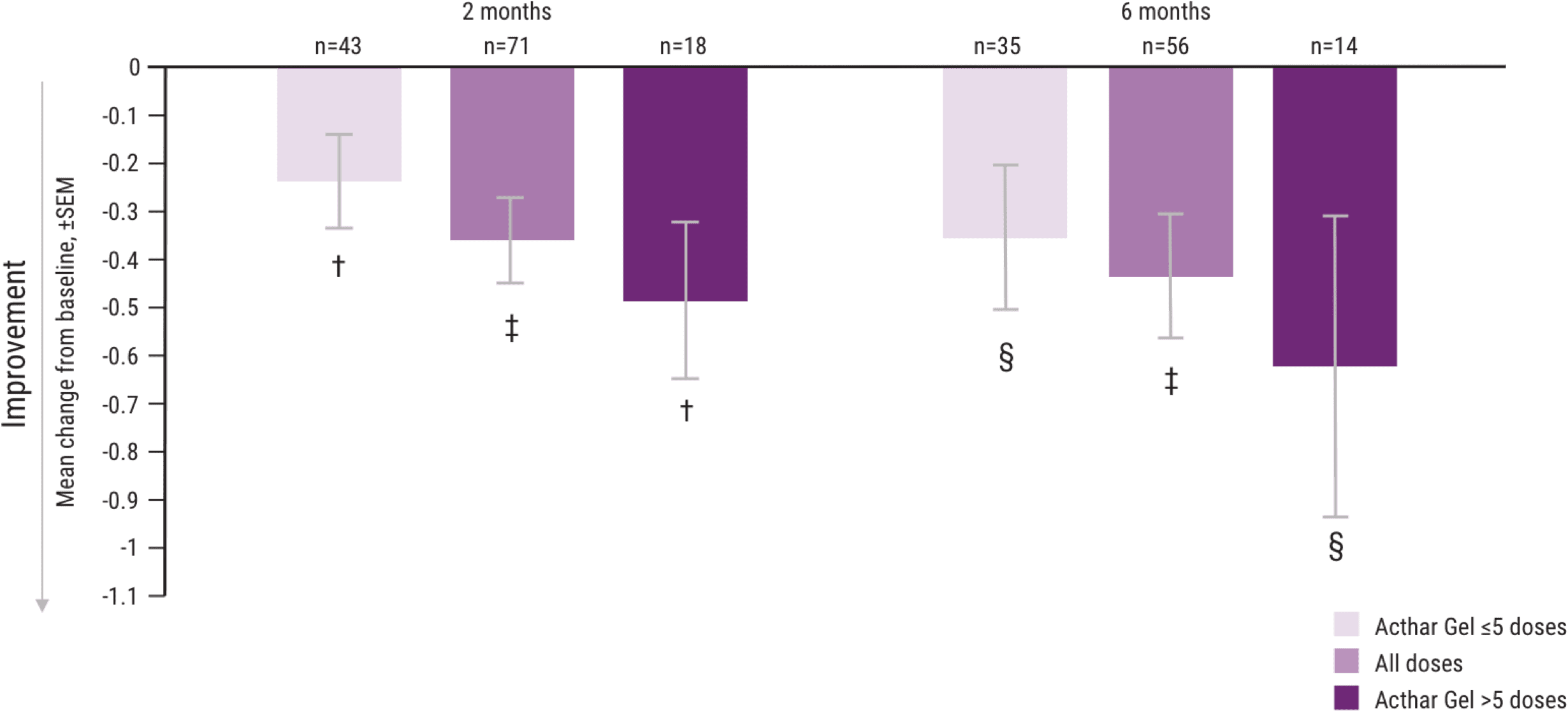
In a post hoc analysis evaluating the number of doses, greater improvements in MSIS-29v1 and EDSS were observed in some patients taking >5 doses of Acthar Gel1
As approved by the FDA, daily intramuscular or subcutaneous doses of 80 to 120 units of Acthar Gel may be administered for 2 to 3 weeks. It may be necessary to taper the dose.9
Mean change from baseline in the MSIS-29v1 physical subscale, by number of doses administered1
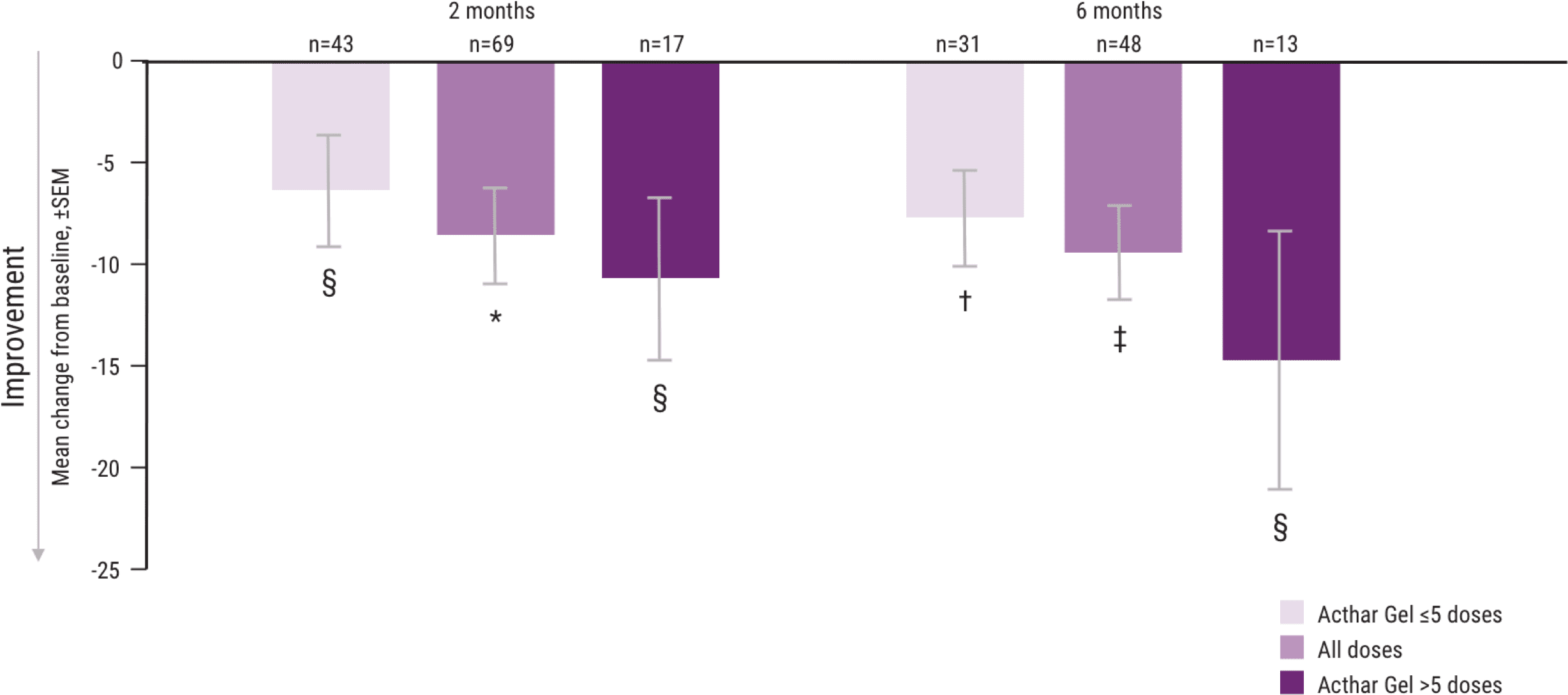
*P <.001.
†P <.01.
‡P <.0001.
§P <.05.
Note: P values are based on Wilcoxon signed rank tests (ITT population) compared with baseline.
Mean change from baseline in the EDSS scale, by number of doses administered1
†P <.01.
‡P <.0001.
§P <.05.
Note: P values are based on Wilcoxon signed rank tests (ITT population) compared with baseline.
Acthar Gel dosing information was collected from patient self-reports.1
AEs and SAEs were consistent with the published label
AE=adverse event; SAE=serious adverse event.
Start the referral process for your appropriate patients

See additional dosing information from clinical experience with Acthar Gel
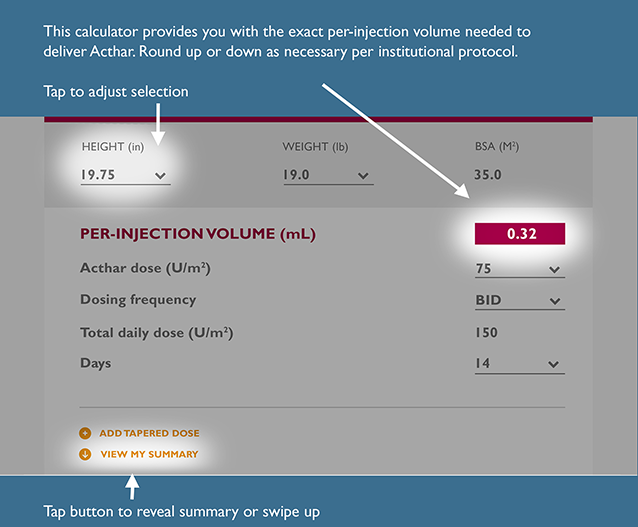
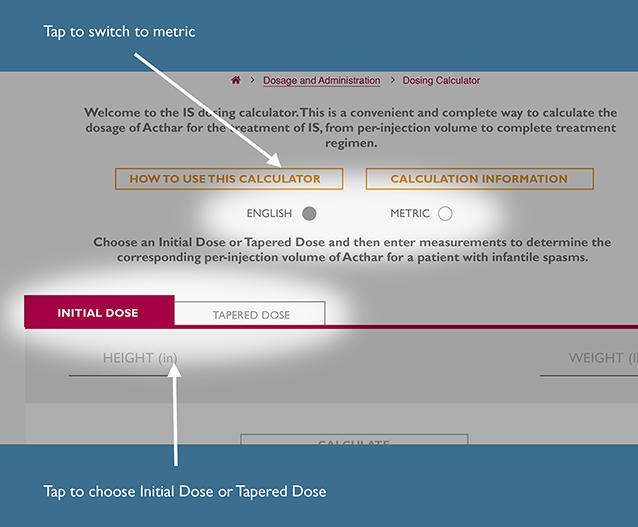
This is a convenient and complete way to calculate the recommended dosage of Acthar Gel for the treatment of IS, from per-injection volume to a complete treatment regimen.
The recommended dosage for IS is 150 units/m2 divided into twice daily intramuscular injections of 75 units/m2 over a 2‑week period. Dosing should be gradually tapered and discontinued over a 2‑week period.
Choose initial dose or tapered dose and then enter measurements to determine the corresponding per-injection volume of Acthar Gel for a patient with IS.
INITIAL DOSE
TAPERED DOSE #1
For Infantile Spasms, the Acthar IS Dosing Calculator generates per-injection volume (mL) of Acthar by body surface area (BSA) using the following Mosteller formula calculation22:
To determine per-injection volume of Acthar:
To determine total daily dose:
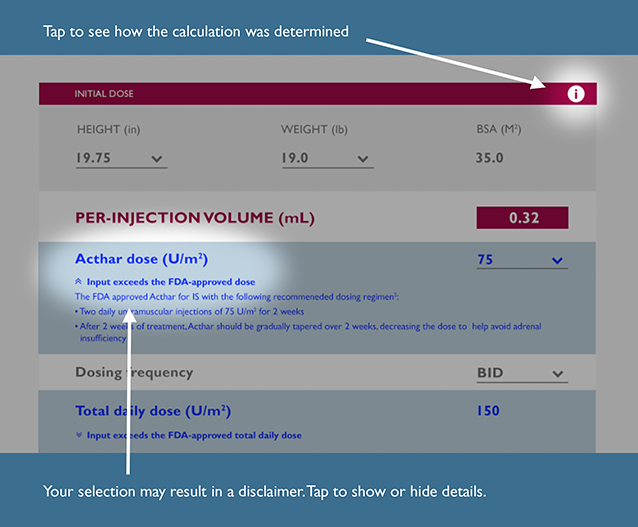
Input exceeds the FDA-recommended dose
The FDA approved Acthar for IS with the following recommended dosing regimen1:
Input is below the FDA-recommended dose
The FDA approved Acthar for IS with the following recommended dosing regimen1:
Input exceeds the preceding total daily dose
After 2 weeks of treatment, Acthar should be gradually tapered, decreasing the dose to help avoid adrenal insufficiency. The FDA approved Acthar for IS with the following recommended taper schedule1:
30 U/m2 in the morning for 3 days; 15 U/m2 in the morning for 3 days; 10 U/m2 in the morning for 3 days; and 10 U/m2 every other morning for 6 days.
The previous dose is outside the FDA-approved recommendation for dose range; therefore, the default taper dose may need assessment
After 2 weeks of treatment, Acthar should be gradually tapered, decreasing the dose to help avoid adrenal insufficiency. The FDA approved Acthar for IS with the following recommended taper schedule1:
30 U/m2 in the morning for 3 days; 15 U/m2 in the morning for 3 days; 10 U/m2 in the morning for 3 days; and 10 U/m2 every other morning for 6 days.
Input differs from the FDA-recommended frequency of treatment
The FDA approved Acthar for IS with the following recommended dosing regimen1:
Input differs from the FDA-approved tapering schedule recommendation
After 2 weeks of treatment, Acthar should be gradually tapered, decreasing the dose to help avoid adrenal insufficiency. The FDA approved Acthar for IS with the following recommended taper schedule1:
30 U/m2 in the morning for 3 days; 15 U/m2 in the morning for 3 days; 10 U/m2 in the morning for 3 days; and 10 U/m2 every other morning for 6 days.
The symptoms of adrenal insufficiency in infants treated for infantile spasms can be difficult to identify. The symptoms are non-specific and may include anorexia, fatigue, lethargy, weakness, excessive weight loss, hypotension and abdominal pain. It is critical that parents and caregivers be made aware of the possibility of adrenal insufficiency when discontinuing Acthar Gel and should be instructed to observe for, and be able to recognize, these symptoms.
Input exceeds the preceding total daily dose
After 2 weeks of treatment, Acthar should be gradually tapered, decreasing the dose to help avoid adrenal insufficiency. The FDA approved Acthar for IS with the following recommended taper schedule1:
30 U/m2 in the morning for 3 days; 15 U/m2 in the morning for 3 days; 10 U/m2 in the morning for 3 days; and 10 U/m2 every other morning for 6 days.
Input exceeds the preceding total daily dose
After 2 weeks of treatment, Acthar should be gradually tapered, decreasing the dose to help avoid adrenal insufficiency. The FDA approved Acthar for IS with the following recommended taper schedule1:
30 U/m2 in the morning for 3 days; 15 U/m2 in the morning for 3 days; 10 U/m2 in the morning for 3 days; and 10 U/m2 every other morning for 6 days.
Input exceeds the FDA-recommended total daily dose
The FDA approved Acthar for IS with the following recommended dosing regimen1:
Please note that there are no data to support the use of Acthar at a total daily dose exceeding 150 U/m2. This dosing calculator is not a substitute for clinical judgment. Medical discretion is required to determine any appropriate daily dose and treatment course of Acthar for your IS patients.
Input is below the FDA-recommended total daily dose
The FDA approved Acthar for IS with the following recommended dosing regimen1:
Input differs from the FDA-recommended days on therapy
The FDA approved Acthar for IS with the following recommended dosing regimen1:
Input differs from the FDA-approved tapering schedule recommendation
After 2 weeks of treatment, Acthar should be gradually tapered, decreasing the dose to help avoid adrenal insufficiency. The FDA approved Acthar for IS with the following recommended taper schedule1:
30 U/m2 in the morning for 3 days; 15 U/m2 in the morning for 3 days; 10 U/m2 in the morning for 3 days; and 10 U/m2 every other morning for 6 days.
The symptoms of adrenal insufficiency in infants treated for infantile spasms can be difficult to identify. The symptoms are non-specific and may include anorexia, fatigue, lethargy, weakness, excessive weight loss, hypotension and abdominal pain. It is critical that parents and caregivers be made aware of the possibility of adrenal insufficiency when discontinuing Acthar Gel and should be instructed to observe for, and be able to recognize, these symptoms.
ADD TAPERED DOSE
REMOVE THIS DOSE
VIEW MY SUMMARY
For infantile spasms, the Acthar IS Dosing Calculator generates per-injection volume (mL) of Acthar by body surface area (BSA) using the following Mosteller formula calculation22:

To determine per-injection volume of Acthar:

To determine total daily dose:
To determine total volume of Acthar required to complete your selected course of treatment:

To determine number of vials needed:

References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References: