Prescribe Acthar Gel now
Start the referral process for your appropriate patients
Hladunewich MA, Cattran D, Beck LH, Odutayo A, Sethi S, Ayalon R, Leung N, Reich H, Fervenza FC—Nephrology Dialysis Transplantation, 2014
Disclosure statement: Funding to support this study was provided by Mallinckrodt Pharmaceuticals.
To assess the safety and efficacy of Acthar Gel in 20 adults (>18 years) with biopsy-proven iMN with proteinuria due to nephrotic syndrome
Primary outcomes included:
Secondary endpoints included the proportion of patients who achieved:
iMN=idiopathic membranous nephropathy.
*Proteinuria <0.3 g/day.
†Reduction in proteinuria by >50% with a final urine protein <3.5 g/day, but >0.3 g/day.
‡Reduction in proteinuria by <50%, or worsening of proteinuria.
At baseline, the mean age of the study population was 51 years and the median disease latency was 14 months. Thirteen of 20 patients had not received previous immunosuppressive agents.
§Significant renal insufficiency was defined as estimated glomerular filtration rate (eGFR) ≥40 mL/min/1.73 m2 while taking RAS blockade.
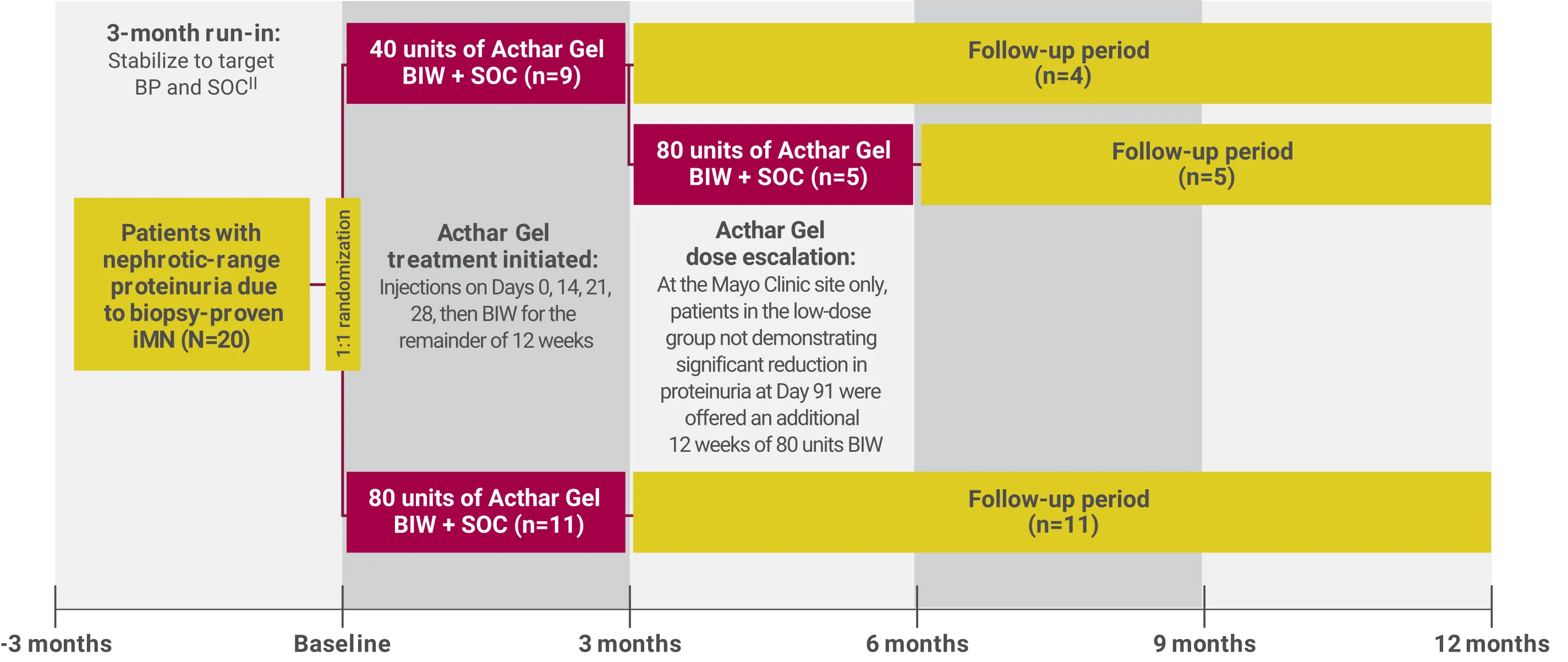
BIW=twice weekly; SOC=standard of care.
||SOC included statin therapy at the maximum recommended dose, dietary counseling to maintain a low-salt diet (2–3 g/day), and a target dietary protein intake of 0.8 g/kg ideal body weight/day of high-quality protein.
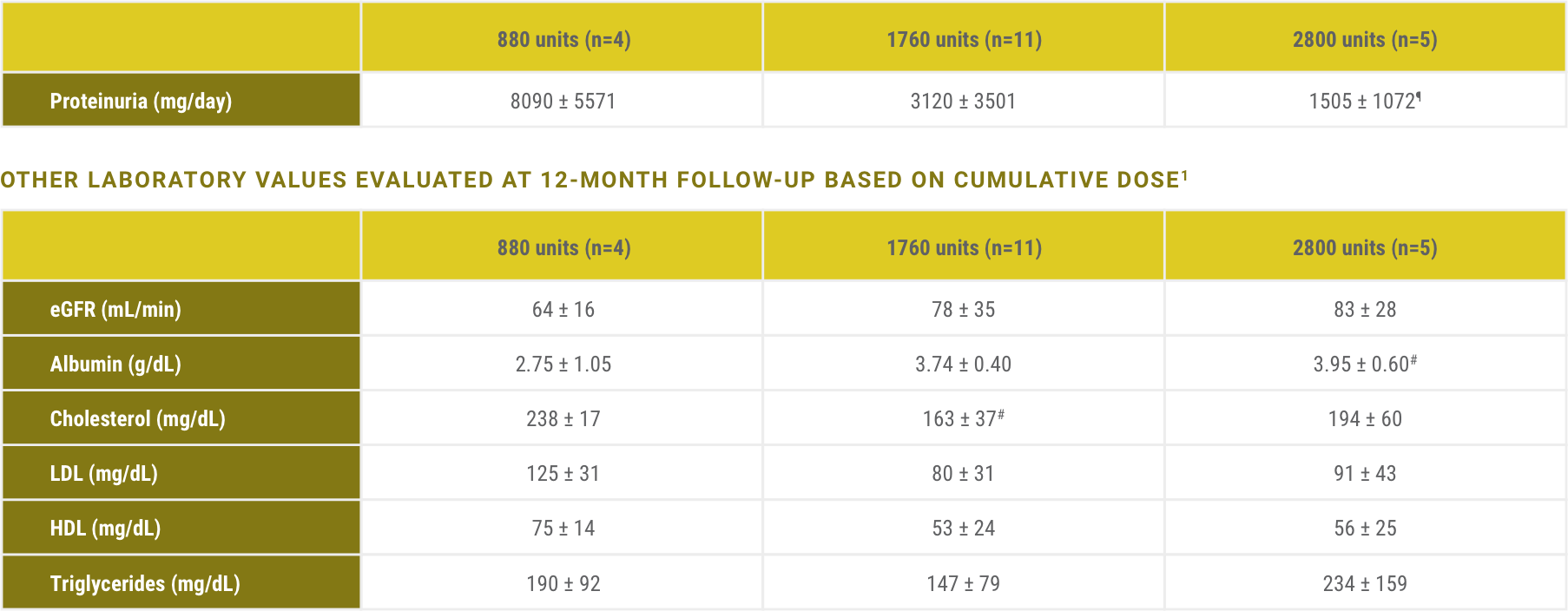
Significant improvement in mean proteinuria was observed at completion of Acthar Gel treatment and 12-month follow-up1
Mean proteinuria improved and was reduced significantly over 12 months, even after Acthar Gel treatment was completed

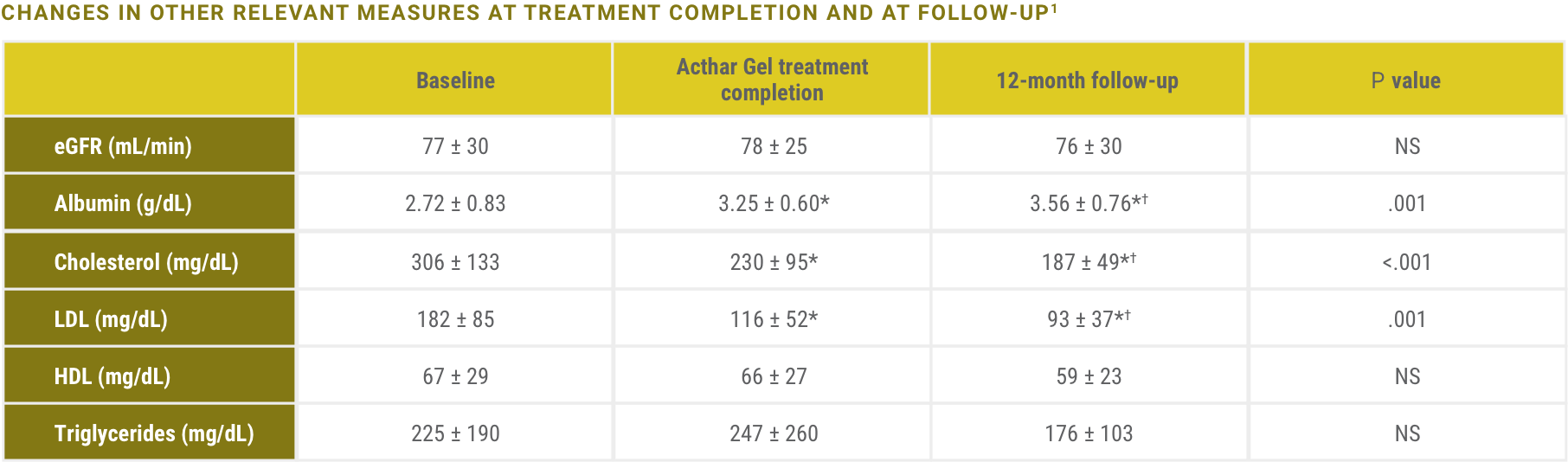
Acthar Gel is indicated to reduce proteinuria in nephrotic syndrome.2 The impact of Acthar Gel on other relevant lab values has not been more formally assessed and is included here for clinical context only.
eGFR=estimated glomerular filtration rate; HDL=high-density lipoprotein; LDL=low-density lipoprotein; NS=not significant.
*P<.05 versus baseline.
†P<.05 versus Acthar Gel treatment completion.
Patients experienced a greater than 50% reduction in proteinuria1

‡Complete remission was defined as proteinuria <0.3 g/day. Partial remission was defined as a reduction in proteinuria by >50% with a final urine protein <3.5 g/day, but >0.3 g/day. No response was defined as a reduction in proteinuria by <50%, or worsening of proteinuria.
§One patient experienced significant improvement in proteinuria, but did not meet criteria for partial remission.
||Of these patients, 2 were given alternate immunosuppression prior to completion of the trial and were excluded from 12-month follow-up data.
Acthar Gel is indicated to reduce proteinuria in nephrotic syndrome. The impact of Acthar Gel on other relevant lab values has not been more formally assessed and is included here for clinical context only.
¶P<.05 for trend across groups.
#P<.05 versus 880 units.
No patient discontinued Acthar Gel therapy due to treatment-related adverse events
The following adverse events occurred during the year of follow-up, but not all cases were clearly related to the therapy: tremulousness (n=3), hoarseness (n=2), dizziness (n=5), muscle aches or pain (n=5), headaches (n=5), gastrointestinal symptoms (n=7), blurred vision (n=2), and generalized weakness or fatigue (n=9).
Transient increases to a blood glucose level ≥130 mg/dL occurred in 5 patients. One patient sustained a clinically important glucose increase and required dietary treatment, which was improved with weight loss.
Start the referral process for your appropriate patients

See additional dosing information from clinical experience with Acthar Gel
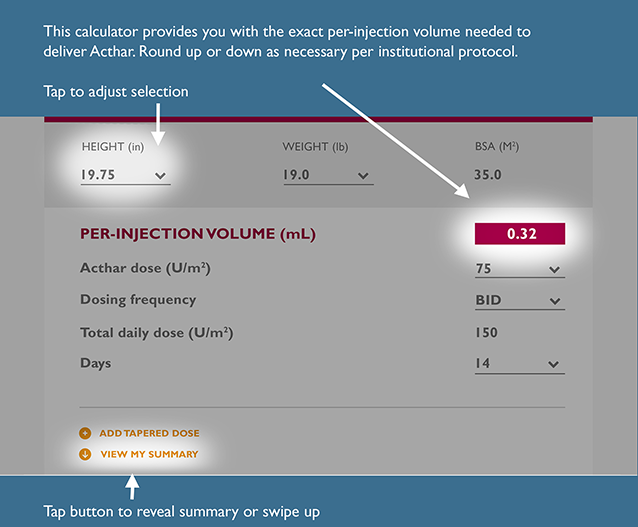
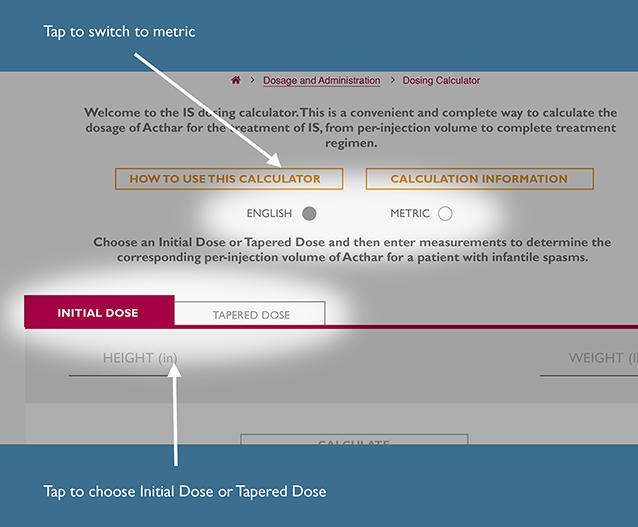
This is a convenient and complete way to calculate the recommended dosage of Acthar Gel for the treatment of IS, from per-injection volume to a complete treatment regimen.
The recommended dosage for IS is 150 units/m2 divided into twice daily intramuscular injections of 75 units/m2 over a 2‑week period. Dosing should be gradually tapered and discontinued over a 2‑week period.
Choose initial dose or tapered dose and then enter measurements to determine the corresponding per-injection volume of Acthar Gel for a patient with IS.
INITIAL DOSE
TAPERED DOSE #1
For Infantile Spasms, the Acthar IS Dosing Calculator generates per-injection volume (mL) of Acthar by body surface area (BSA) using the following Mosteller formula calculation22:
To determine per-injection volume of Acthar:
To determine total daily dose:
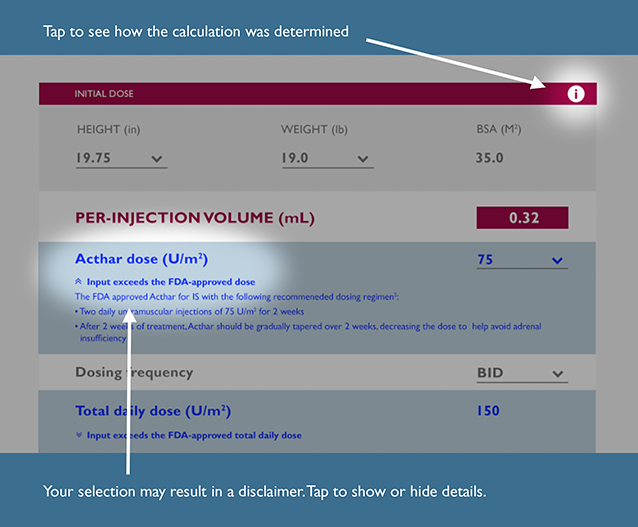
Input exceeds the FDA-recommended dose
The FDA approved Acthar for IS with the following recommended dosing regimen1:
Input is below the FDA-recommended dose
The FDA approved Acthar for IS with the following recommended dosing regimen1:
Input exceeds the preceding total daily dose
After 2 weeks of treatment, Acthar should be gradually tapered, decreasing the dose to help avoid adrenal insufficiency. The FDA approved Acthar for IS with the following recommended taper schedule1:
30 U/m2 in the morning for 3 days; 15 U/m2 in the morning for 3 days; 10 U/m2 in the morning for 3 days; and 10 U/m2 every other morning for 6 days.
The previous dose is outside the FDA-approved recommendation for dose range; therefore, the default taper dose may need assessment
After 2 weeks of treatment, Acthar should be gradually tapered, decreasing the dose to help avoid adrenal insufficiency. The FDA approved Acthar for IS with the following recommended taper schedule1:
30 U/m2 in the morning for 3 days; 15 U/m2 in the morning for 3 days; 10 U/m2 in the morning for 3 days; and 10 U/m2 every other morning for 6 days.
Input differs from the FDA-recommended frequency of treatment
The FDA approved Acthar for IS with the following recommended dosing regimen1:
Input differs from the FDA-approved tapering schedule recommendation
After 2 weeks of treatment, Acthar should be gradually tapered, decreasing the dose to help avoid adrenal insufficiency. The FDA approved Acthar for IS with the following recommended taper schedule1:
30 U/m2 in the morning for 3 days; 15 U/m2 in the morning for 3 days; 10 U/m2 in the morning for 3 days; and 10 U/m2 every other morning for 6 days.
The symptoms of adrenal insufficiency in infants treated for infantile spasms can be difficult to identify. The symptoms are non-specific and may include anorexia, fatigue, lethargy, weakness, excessive weight loss, hypotension and abdominal pain. It is critical that parents and caregivers be made aware of the possibility of adrenal insufficiency when discontinuing Acthar Gel and should be instructed to observe for, and be able to recognize, these symptoms.
Input exceeds the preceding total daily dose
After 2 weeks of treatment, Acthar should be gradually tapered, decreasing the dose to help avoid adrenal insufficiency. The FDA approved Acthar for IS with the following recommended taper schedule1:
30 U/m2 in the morning for 3 days; 15 U/m2 in the morning for 3 days; 10 U/m2 in the morning for 3 days; and 10 U/m2 every other morning for 6 days.
Input exceeds the preceding total daily dose
After 2 weeks of treatment, Acthar should be gradually tapered, decreasing the dose to help avoid adrenal insufficiency. The FDA approved Acthar for IS with the following recommended taper schedule1:
30 U/m2 in the morning for 3 days; 15 U/m2 in the morning for 3 days; 10 U/m2 in the morning for 3 days; and 10 U/m2 every other morning for 6 days.
Input exceeds the FDA-recommended total daily dose
The FDA approved Acthar for IS with the following recommended dosing regimen1:
Please note that there are no data to support the use of Acthar at a total daily dose exceeding 150 U/m2. This dosing calculator is not a substitute for clinical judgment. Medical discretion is required to determine any appropriate daily dose and treatment course of Acthar for your IS patients.
Input is below the FDA-recommended total daily dose
The FDA approved Acthar for IS with the following recommended dosing regimen1:
Input differs from the FDA-recommended days on therapy
The FDA approved Acthar for IS with the following recommended dosing regimen1:
Input differs from the FDA-approved tapering schedule recommendation
After 2 weeks of treatment, Acthar should be gradually tapered, decreasing the dose to help avoid adrenal insufficiency. The FDA approved Acthar for IS with the following recommended taper schedule1:
30 U/m2 in the morning for 3 days; 15 U/m2 in the morning for 3 days; 10 U/m2 in the morning for 3 days; and 10 U/m2 every other morning for 6 days.
The symptoms of adrenal insufficiency in infants treated for infantile spasms can be difficult to identify. The symptoms are non-specific and may include anorexia, fatigue, lethargy, weakness, excessive weight loss, hypotension and abdominal pain. It is critical that parents and caregivers be made aware of the possibility of adrenal insufficiency when discontinuing Acthar Gel and should be instructed to observe for, and be able to recognize, these symptoms.
ADD TAPERED DOSE
REMOVE THIS DOSE
VIEW MY SUMMARY
For infantile spasms, the Acthar IS Dosing Calculator generates per-injection volume (mL) of Acthar by body surface area (BSA) using the following Mosteller formula calculation22:

To determine per-injection volume of Acthar:

To determine total daily dose:
To determine total volume of Acthar required to complete your selected course of treatment:

To determine number of vials needed:

References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References:
References: